'%3e%3ctitle%3eminefield%3c/title%3e%3cpath d='M13.6 4l-4 11.2-9.6-6.4 3.2 10.4c0.736 2.368 1.6 2.4 3.2 2.4h3.2v-1.6h8v1.6h3.2c1.6 0 2.4-0.704 3.2-2.4l3.2-10.4-9.6 6.4-4-11.2zM11.2 21.6v1.6c-3.552 0-6.4 1.056-6.4 2.4s2.848 2.4 6.4 2.4h4.8c3.552 0 6.4-1.088 6.4-2.4s-2.848-2.4-6.4-2.4v-1.6h-4.8z'/%3e%3c/svg%3e)
Dr. Thomas Antone, DC, AMD
Doctor of Chiropractic, Alternative Medical Doctor, Neurofeedback Therapist, Hyperbaric Oxygen Therapy Clinician
SOFT or HARD Chamber?
SOFT CHAMBER OR HARD CHAMBER?
What is the difference?
Let’s look at some questions: What are they made of and why? What is the comparison? Which is more effective? What official requirements?
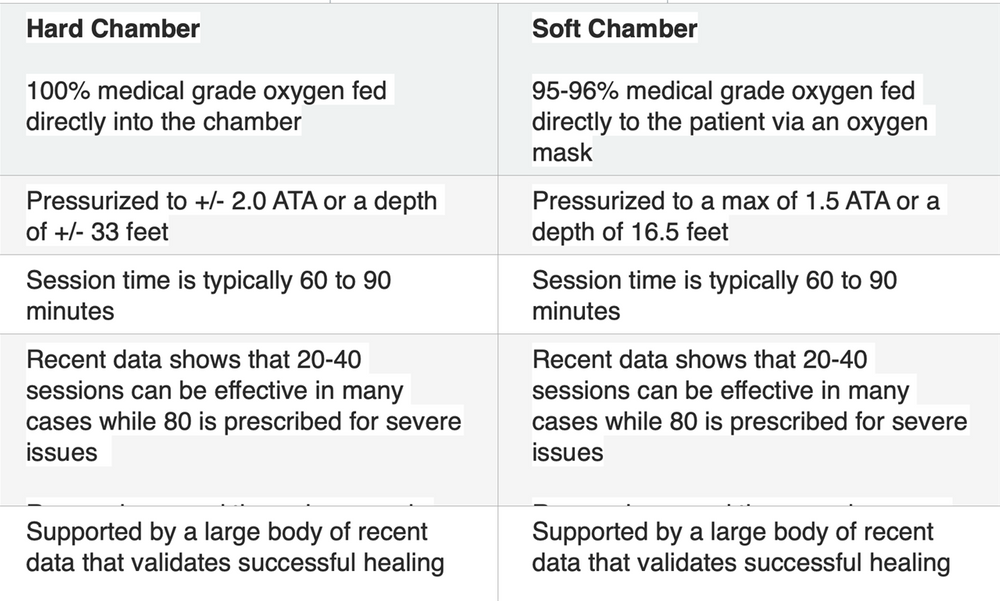
SOFT CHAMBER OR HARD CHAMBER? What is the difference? Let’s look at some questions: What are chambers made of and why? What is the comparison [dollars & benefits]?; Which one is more effective overall?; and What are the official requirements to install one or the other in your facility or home? [Note: ATA means “At Absolute” and though not technically correct, is commonly used as the average atmospheric pressure or ATM at sea level, equaling 14.7 psi. For chamber pressures, this ‘ambient’ pressure is subtracted from the total: Thus, 2 ATA = 14.7 psi, 1.41 ATA = 6 psi of (added) pressure inside the chamber.]
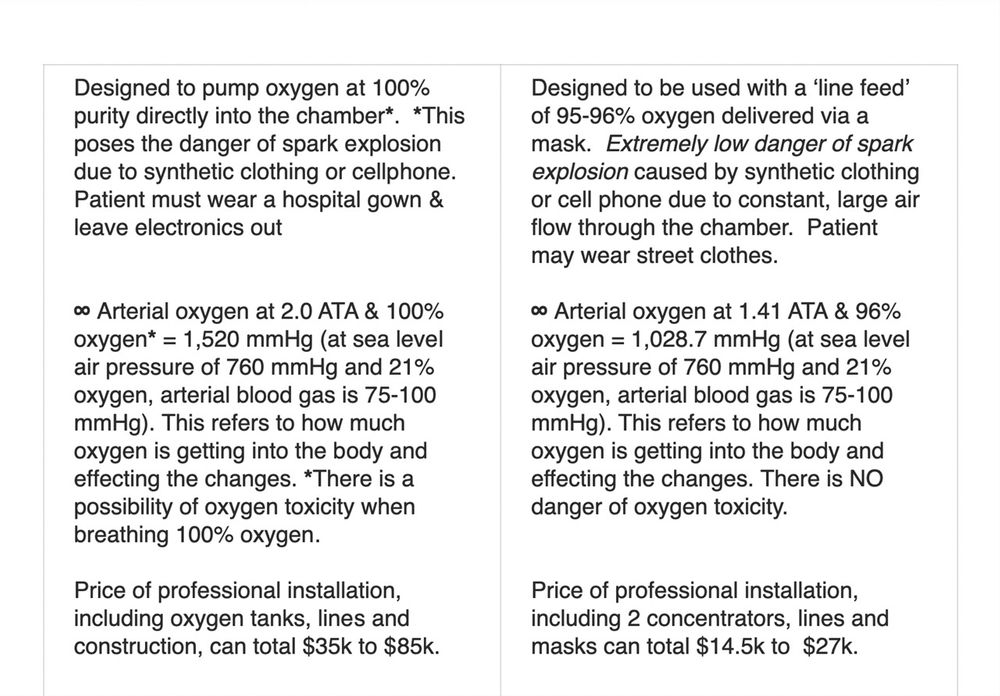
What are they made of and why? Monoplace (single person) Hard chambers are either made of transparent acrylic, aluminum or stainless steel. These materials are best suited to handle the high pressures used for most of the 13 extreme conditions listed by Medicare as approved for HBOT. In addition, when operated thusly they require that oxygen (usually at a purity of 100%) be delivered via an equally high pressure system - either directly into the chamber or via a hood or, rarely, a mask. This requires a large oxygen tank or tanks to be installed outside the building, surrounded by a cinderblock enclosure to ensure that, in the event of explosion, the violent discharge can be contained. Thus, it requires adherence to the National Fire Protection Association (NFPA-99) regulations and must be approved by your local fire department and inspected regularly. In addition, any neighbor within a prescribed distance must be notified and approve of the tanks.
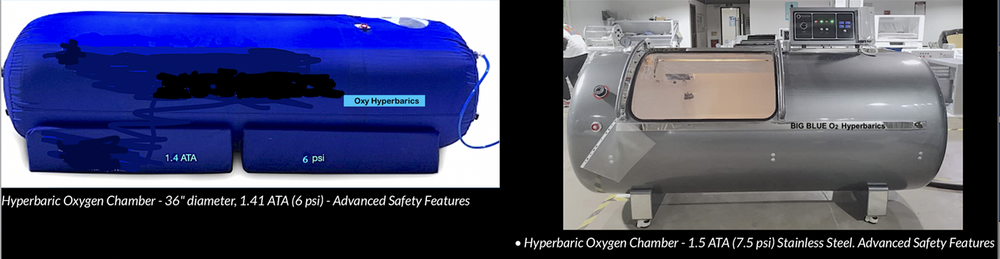
Monoplace (single person) Soft chambers are typically made of high-strength, double- sided, 44 oz Medical Grade, Urethane Coated, non-toxic TPU (Thermoplastic PolyUrethane) with interwoven Dacron fibers. This material was pioneered by NASA for use in their early space suits. It is slightly flexible while retaining its strength and feels as hard as steel when inflated. Each chamber made of this material is thoroughly tested at pressures up to 1.7 ATA (10.29 psi), however the mfg recommended pressures are between 1.3 ATA (4.4 psi) and 1.5 ATA (7.5 psi). This is due to the fact that the heavy duty zippers and small acrylic windows are more susceptible to failure at high pressures than is the chamber material. They can be safely operated using an Oxygen Concentrator (or two) that provides 95-96% pure oxygen at a flow rate of 10 liters per minute and an output pressure of 20 psi. This method is effective (see below) and safe because the concentrators can be in the room with the chamber and there’s no danger of explosion. Two concentrators in parallel provide enough pressure for the Oxygen delivered inside a 6 psi chamber to sustain a flow of +/- 12 lpm & 95-96% O2 while inflated. No permits or neighbor notifications are necessary.
What is the comparison, ‘per-dollar’?
Many Hyperbaric Centers use hard chambers that operate at high pressures (1.5 to 3.0 ATA) exclusively, as they try to emulate the “medical (hospital) model” even though they cost between approximately $26k to $75k for 1 chamber alone; and the benefits are only modestly more than soft chambers (see below). Add to that the cost of oxygen tanks, enclosure, special through-the-wall tubing, oxygen gas refills, liability insurance, etc and the cost is quite prohibitive. This translates into high per-session fees for the patient and with only about 13 approved conditions that are reimbursable by Medicare or (sometimes) private insurance, the patient is left with high out-of-pocket expenses.
Soft chambers range in price between approximately $9k and $23K. Most of these are the 1.3 ATA (4.4 psi) type with a couple of companies offering the 1.41 ATA (6 psi) type. As stated above, there are few extra costs*, no construction costs, no regulatory licenses and no extra insurance to cover explosion liability. This translates into lower per- session fees for the patient and the possibility of insurance coverage for certain approved conditions outside of those stipulated by Medicare (the Medical Model standard). *A high- power, high-purity oxygen concentrator will cost between $1,500 and $2,400 and 50 oxygen masks will cost approximately $100.
Which one is more effective, overall?
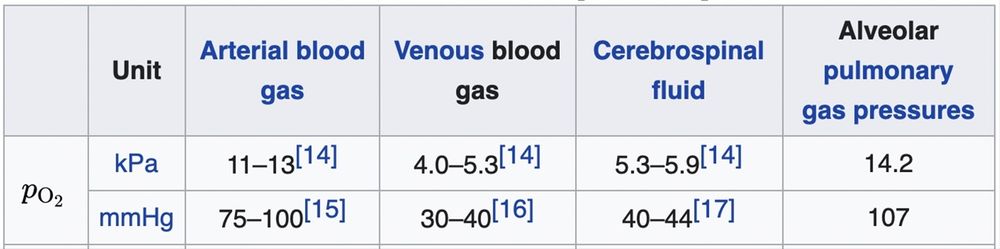
The vast majority of patients using Hard and soft chambers are getting the success they seek from HBOT for various issues that are not on the list of ‘approved’ conditions. These range from TBI (Concussion) to Age Reduction to Sports Injury and Chronic Inflammation, to name a few. With that said, the question of pressure and Oxygen purity becomes relevant. It’s all about the partial pressure of gasses - (Dalton's Law): “In a mixture of gases, each constituent gas has a partial pressure which is the putative pressure of that constituent gas if it alone occupied the entire volume of the original mixture at the same temperature. The partial pressure of Oxygen is notated as PO2. [See chart below for some PO2 readings at certain body locations at 1 ATA] Henry's law is a gas law that states that, “The amount of dissolved gas in a liquid is proportional to its partial pressure above the liquid.” [See ∞ in comparison chart, above]
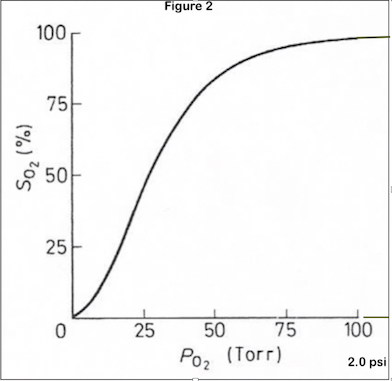
How HBOT works: ‘Diffusive transport’ is the passive movement of oxygen across several barriers, such as the endothelium, the alveolus and the mitochondrial membrane. The amount of diffusive oxygen movement depends on the gradient of partial pressure of oxygen, the available surface area to diffusion, the permeability and thickness of diffusion barriers and the local metabolic demand. The diffusion of hemoglobin (its oxygen saturation) increases rapidly from 1 ATA to about 1.4 ATA and then begins to slow in a ‘bell curve’ that almost levels out after that. [See Fig 2 below]. As stated by Dr. Susan Sprau, MD, at UCLA Health, "The pressure that must be achieved is >1.4 ATA. Anything else is not considered Hyperbaric Oxygen."
Tissue partial pressure of oxygen (PO2) is regulated by blood flow, the availability of oxygen and the consumption rate from one region to another. The Bohr effect allows that hemoglobin releases more oxygen in response to the metabolic rate of that tissue which is then limited by the person’s hematocrit (% of red blood cells). For instance, highly metabolic neurons and cardiac myocytes are largely aerobic and depend on the presence of oxygen for their survival, although some lactate can be produced within the brain, most of its cells depend upon the metabolic rate of oxygen consumption alone. The bain is only about 2% of a human's body weight but requires over 25% of available oxygen.
Once oxygen reaches the cells, the gradient of partial pressure of oxygen, from the extracellular space into the cell determines the availability of oxygen to the mitochondria. In highly aerobic cells, such as neurons, energy production depends largely on the availability of oxygen supplied to the mitochondria. Inside this organelle, a series of enzyme-catalysed chemical reactions occur, converting metabolites into carbon dioxide and water to generate usable energy in the form of high-energy phosphates such as ATP (Adenosine Tri-Phosphate).
The mitochondrion PO2 is very small - 1 to 10 mmHg, hence the ease in which HBOT can infuse large amounts of O2 into this area, both as a gas and as a solution carried by plasma, independent of the hematocrit.
As you can see, it doesn’t take much pressure to vastly exceed the PO2 in various parts of the body and effect the positive changes that are evident with this diffusion using Hyperbaric Oxygen Therapy at modest pressures.
Let’s compare some differences by looking at the effect of HBOT on the oxygen in blood, using arterial blood gases. (see chart, below)
The PO2 of arterial oxygen in a chamber at 2.0 ATA (14.7 psi) & 100% oxygen is 1,520 mmHg. (Remember, 1 ATA is 14.7 psi but we subtract that from the chamber’s stated pressure of 2 ATA, leaving 14.7 psi as the ‘added’ or effective pressure.) Air at 1 ATA (sea level) equals a pressure of 760 mmHg & contains 21% oxygen, bringing arterial PO2 (notated as PaO2) to 75-100 mmHg. So, 1,520 mmHg is 15 times normal PaO2.
At 1.41 ATA (6 psi) & 96% oxygen the PaO2 is 1,028.7 mmHg. That’s 10.25 times normal. This equates to a modest difference between Hard & Soft chambers (at these pressures) of 491 mmHg, or 32%. That 32% difference is not statistically significant due to the ‘bell curve’ saturation gradient noted above and seen below in figure 2.
It is clear from the above explanations that HBOT at either of these pressures and oxygen concentrations can result in high levels of oxygen being made available to the body to make the positive changes being reported in current data.
Conclusion
Although hard chambers, providing high pressures & 100% O2, can be modestly (32%) more effective in the initial phases of remediation of some severe cellular damage, soft chambers, running at moderate pressures & 95-96% O2, can provide all that is necessary to continue the healing of these issues - or - initiate and continue the healing of many other severe to chronic issues. We hope this has helped your understanding of the differences between hard and soft hyperbaric oxygen chambers. .